by Dr. Saman Nazir
One in five babies comes into the world by the cesarean section (C-Section) in Pakistan. The most recent report of Pakistan Demographic and Health Survey (PDHS) shows a rapid increase in the rates of C-Section deliveries, from 14% in 2012-13 to 22% in 2017-18. Is the C-Section rate too high in Pakistan? The answer would be a definite YES. World Health Organization, in its statement, recommends that C-Section rates higher than 10% are not associated with a reduction in maternal or neonatal mortality (WHO, 2015). Current rates exceed the World Health Organization recommendations, suggesting that Pakistan is part of a trend worldwide of having C-Sections for non-medical reasons.
Why are we concerned about high C-Section rates? There are four primary reasons. First, extensive use of C-Section can increase the probability of negative impacts on mother and child physical and mental health. A review of seventy-nine studies comparing outcomes of C-Section deliveries versus normal deliveries show that C-Section deliveries are considered at high risk of future medical complications (Jose et al., 2007).
Second, we still have high fertility; the total fertility rate is 3.6 births per woman in Pakistan. With no health records available for previous births, a normal delivery after the C-Section trial gets risky. Having a previous C-Section puts the mother at a higher risk of C-Section for subsequent births. With these high rates of C-Section in the country, we are unduly exposing women to major surgery for multiple times.
Third, Pakistan is a resource-poor country. At times, patients seeking pubic health care do not get common antibiotics from hospitals dispensaries. Spending resources on a surgical procedure for non-medical reasons should be a grave concern for health policymakers, managers, and practitioners.
Fourth, high rates of C-Section in any country could be due to two reasons; either the maternal health care sector is augmenting the C-Section rates for financial gains or medically unnecessarily performing it on women’s choice. In Pakistan, where no hospital, be it public or private, has an explicit pro-choice C-Section policy, the former is deemed to be the case. Moreover, the literature suggests that women have a negative opinion about having a C-Section in Pakistan (Bano et al., 2015; Qazi et al., 2013). Performing C-Section on non-medical reasons for financial gains or time management indicates mal-practicing at the physicians end.
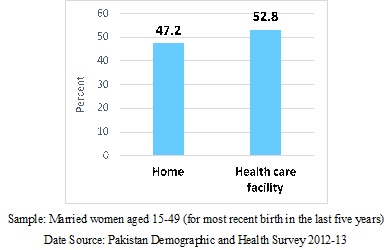
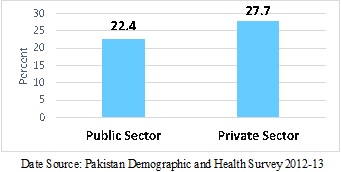
What exactly is happening in Pakistan? Who is responsible for augmenting C-Section rates in the country? In a collaborated research on the medicalization of childbirth in Pakistan, we have explored these questions by using the PDHS. The health care system in Pakistan is predominantly private: about 64% of health expenditure in the country is funded by the private sector (Pakistan Bureau of Statistics, 2018). In our study sample, 53% of the women delivered at the health facility (Figure 1), whereas the C-Section rate in private health facilities was almost 28% (Figure 2).
Elevated rates of C-Section delivery in public health facilities have been explained by the significant number of referrals from periphery public facilities; however, the reason for high rates in private health facilities is less obvious. Therefore, we speculated that private health facilities in Pakistan might be more accommodating of C-Sections for non-medical reasons than public ones.
The findings of our study suggest that medical risk factors, population characteristics, and community socioeconomic status are important factors determining women’s ability to utilize a formal health care system. Medical risk factors are significant at the health facility level to influence the chances of C-Section. We further found that women who deliver at private health facilities are more likely to have a C-Section than women who deliver at public health facilities. The finding is concerning and suggests that the private health sector in Pakistan is over-medicalizing childbirth.
In the private maternal health sector, where gynecologists, obstetricians, and staff are in charge of one-to-one care of pregnant women, they mostly have the sole authority to make medical decisions based on patient conditions. Most likely private maternal care health facilities are preforming C-Sections to earn profits. In public hospitals, there is no economic incentive for doctors to perform a C-Section. However, the doctor’s fee to perform a C-Section and inpatient hospital charges after the procedure are tremendously high (and variable depends upon the facility type and location) in private health facilities in Pakistan. Thus, the findings of the study call for the need for systematic auditing of private maternal health care facilities.
References
Bano, R. et al. (2015). Rates of cesarean section and trials and success of vaginal birth after cesarean sections in secondary care hospital. Journal of Pakistan Medical Association, 65(1), 81-3.
José, M., Althabe, F., & Cafferata, L. M. (2007). Commentary: Health Consequences of the Increasing Cesarean Section Rates. Epidemiology, 18(4), 485–486.
Pakistan Bureau of Statistics (2018). National Health Accounts Pakistan 2015-16. Government of Pakistan Statistics Division. Retrieved from http://www.pbs.gov.pk/sites/default/files//NHA-Pakistan%202015-16%20Report_0.pd
Qazi, Q, Z. Akhtar, K. Khan, and A. H. Khan. (2013). Pregnant Women View Regarding Cesarean Section in Northwest Pakistan. Tropical Medicine and Surgery, 1(1).
World Health Organization. (2015) WHO Statement on Caesarean Section Rates. Geneva: World Health Organization, 2015. WHO/RHR/15.02.
Doctors should first go for normal delivery in Pakistan private sector hospitals.
In Pakistan in majority of cases women go through a c section due to capital gains.
Even if a women insisted on natural child birth, they are scare mongured in to having a c section.
They would be told if you don’t take action you will lose your child.
Out of fear, of loss of a child they take that unfortunate and rushed decision.
There needs to be more self eduction out there to make decisions.
They choices need to be made according to the well being of the mother and child by an experienced practitioner.
In Pakistan most of obstetricians perform early ARM (Artificial Rupture of Membranes) for poor outcome through vaginal delivery in case patient or attendent refuse for c-section.
Epidemics in Pakistan pose significant public health challenges, requiring swift and coordinated responses from authorities.
Effective measures such as robust surveillance, vaccination campaigns, and community education are crucial in controlling outbreaks.
Collaboration between government agencies, healthcare providers, and communities is essential to mitigate the impact of epidemics and protect public health.